
Understanding advanced cancer.
FixCancer.org is a plain-language educational resource. It explains what cancer is, how it is staged, the main types of treatment, and how clinical trials and investigational research work. Every section draws on public information from the National Cancer Institute and other government and nonprofit sources.
This site is educational. It is not medical advice, it does not diagnose or treat any condition, it does not offer or arrange any treatment, and it does not recommend any therapy. People with questions about their own care should talk with a licensed physician.
- Educational Information
- Sources Cited
- Not Medical Advice
- No Treatment Offered
Educational information, not medical advice.
Nothing on this page is a diagnosis, a treatment plan, or a recommendation for any specific therapy. Cancer care is highly individual. Decisions about testing, staging, and treatment are made by a licensed treating physician who knows the full medical picture. If you or someone you love has cancer, bring questions from this page to your own care team.
What cancer is.
Cancer is a group of diseases in which some of the body’s cells grow without normal control and can spread into nearby tissue. The body is made of trillions of cells. Normally cells grow, divide, and die in an orderly way. In cancer, that process breaks down. Damaged or abnormal cells survive when they should die, and new cells form when the body does not need them.
How cancer differs from normal growth.
Cancer cells differ from normal cells in several ways. They can ignore signals that tell cells to stop dividing or to die. They can influence nearby normal cells to form blood vessels that feed a tumor. They can also hide from the immune system. These changes are driven by alterations in genes that control how cells function, especially how they grow and divide.
Solid tumors and blood cancers.
Most cancers form solid tumors, which are masses of tissue. Cancers of the blood, such as leukemias, generally do not form solid tumors. Cancers are usually named for the organ or tissue where they form, such as breast cancer or lung cancer, or for the type of cell that formed them, such as a carcinoma, which begins in epithelial cells, or a sarcoma, which begins in bone or soft tissue.
Source for this section: National Cancer Institute, “What Is Cancer?” See the references below for links.
Understanding cancer stages.
Staging describes how much cancer is in the body and where it is located. Doctors use staging to plan treatment and to talk about a person’s outlook. Many solid tumors are grouped into stages 0 through IV, often using the TNM system, which records the size of the tumor (T), whether it has reached nearby lymph nodes (N), and whether it has spread to distant parts of the body (M).
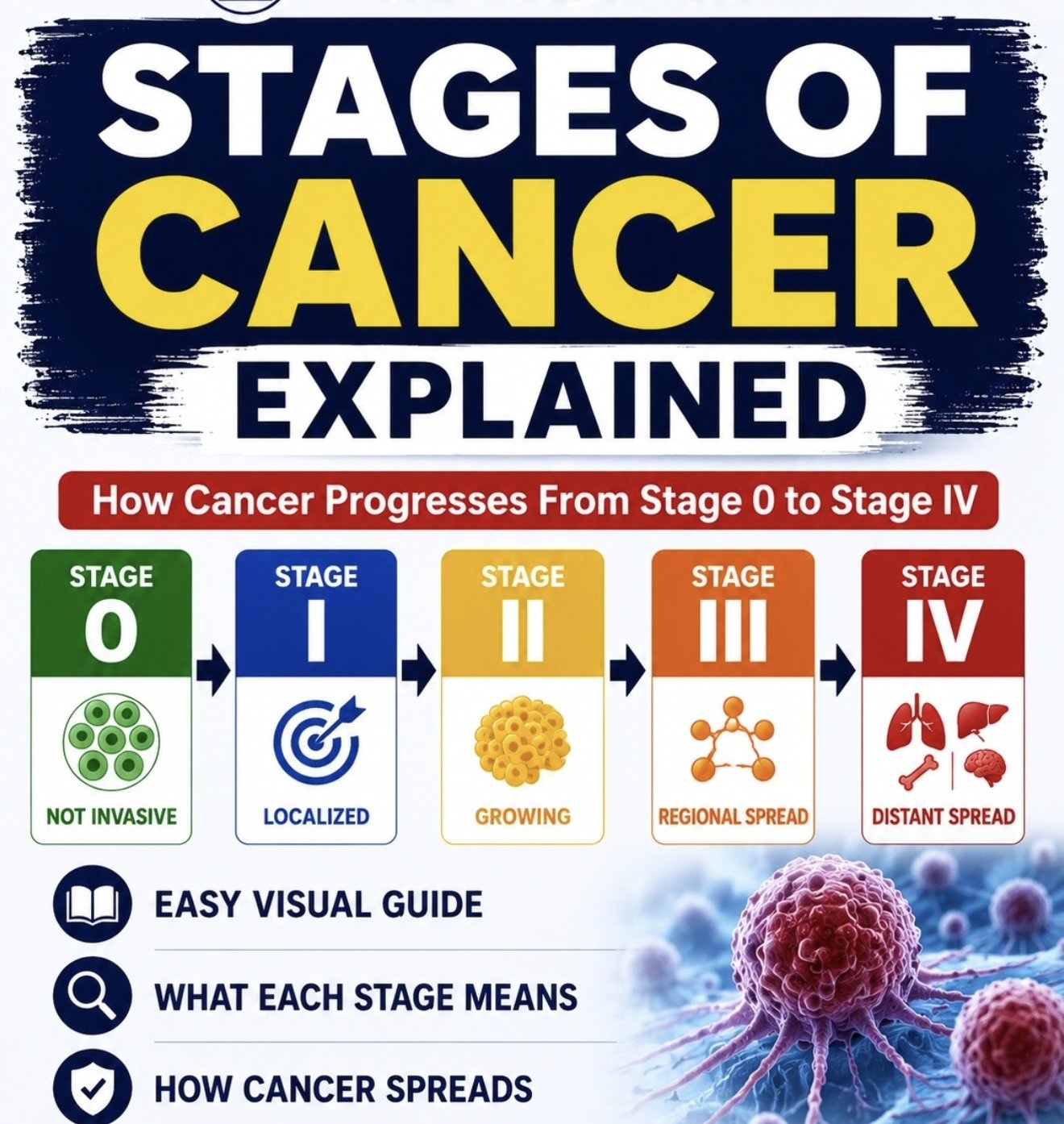
What the numbers mean
- Stage 0: abnormal cells are present but have not spread. Often called carcinoma in situ.
- Stages I, II, and III: cancer is present. Higher numbers mean a larger tumor or more spread into nearby tissue or lymph nodes.
- Stage IV: cancer has spread to distant parts of the body. This is also called metastatic cancer.
Why staging matters
- It helps the care team choose among surgery, radiation, drug therapy, and other options.
- It provides a common language so different specialists describe the same situation the same way.
- It is one input among many. A person’s overall health and the specific biology of the cancer also matter.
Advanced and metastatic cancer.
“Advanced cancer” is a general term for cancer that is unlikely to be cured. It often refers to cancer that has spread from where it started to other parts of the body. When cancer spreads, the new tumors are called metastases. Metastatic cancer keeps the name of the original cancer. Breast cancer that spreads to the lung is still called metastatic breast cancer, not lung cancer.
What advanced cancer care focuses on.
For many people with advanced cancer, the goals of care shift toward controlling the cancer for as long as possible, easing symptoms, and protecting quality of life. Treatment may still slow the cancer or shrink tumors. Palliative care, which focuses on comfort and support, can be provided alongside treatments that target the cancer itself.
Treatment is individual.
There is no single approach to advanced cancer. The right plan depends on the type of cancer, where it has spread, prior treatments, the person’s overall health, and their own goals and preferences. These decisions belong with a licensed oncology team. This page explains general concepts so that conversations with that team can be more informed.
The main types of cancer treatment.
There are many kinds of cancer treatment. The types used depend on the cancer and how advanced it is. Many people receive a combination. The descriptions below are general education, not recommendations.
Local treatments
- Surgery removes the tumor and sometimes nearby tissue.
- Radiation therapy uses high doses of energy to kill cancer cells or shrink tumors in a targeted area.
- Ablation and other local techniques destroy small tumors with heat, cold, or other energy.
Systemic treatments
- Chemotherapy uses drugs to kill or slow fast-growing cells throughout the body.
- Targeted therapy acts on specific changes in cancer cells.
- Immunotherapy helps the immune system find and attack cancer.
- Hormone therapy slows cancers that use hormones to grow.
Supportive care
- Palliative care manages symptoms and side effects at any stage.
- Clinical trials may offer access to treatments under study.
- Survivorship and supportive services address nutrition, mental health, and recovery.
Source for this section: National Cancer Institute, “Types of Cancer Treatment.” Whether any treatment is appropriate for a given person is decided by that person’s licensed physicians.
How clinical trials work.
Clinical trials are research studies that involve people. In cancer, they test whether a new treatment, or a new way of using an existing treatment, is safe and works well. Trials are how investigational ideas become standard care. Every cancer treatment used today was first studied in clinical trials.
The phases of a trial.
Treatment trials usually move through phases. Phase 1 studies test whether a new approach is safe and how it should be given, in a small group of people. Phase 2 studies look at whether it has an effect on a specific cancer. Phase 3 studies compare the new approach with the current standard of care in larger groups. Phase 4 studies continue to study a treatment after it is approved.
Protections for participants.
Clinical trials follow a detailed plan called a protocol and are reviewed by an institutional review board to help protect participants. People who join give informed consent, which means they receive clear information about what the study involves, its possible risks and benefits, and their right to leave at any time.
Finding registered trials.
In the United States, many trials are listed on ClinicalTrials.gov, a public registry maintained by the National Institutes of Health. A person and their physician can search it to see what studies exist for a specific cancer and where they are offered.
Investigational research, explained.
“Investigational” means a treatment or idea is still being studied and has not been approved by the U.S. Food and Drug Administration as safe and effective for general use. Investigational research is an early part of the long path described above. Findings in the laboratory or in animals do not establish that something is safe or effective in people. Reading about investigational science is useful for understanding where research is headed. It is not a basis for personal medical decisions.
One example: Targeted Osmotic Lysis (TOL)
Targeted Osmotic Lysis is an investigational, research-stage mechanism that has been studied in laboratory and veterinary models. The published scientific hypothesis examines the activity of voltage-gated sodium channels on solid tumor cells. TOL is not approved by the FDA, its safety and effectiveness in humans are not established, and the human evidence is limited to individual case reports, only one of which is indexed in PubMed. There are no human trials of TOL registered on ClinicalTrials.gov.
This site describes TOL strictly as investigational science for educational purposes. It does not present TOL as a treatment, does not describe how any treatment would be given, makes no claim of benefit, and does not offer, arrange, or refer anyone for it. Readers interested in the underlying research can review the peer-reviewed literature directly.
Verifiable references on PubMed include PMID 35453588, PMID 36230549, PMID 29643996, PMID 32486340, PMID 35967596, PMID 34201380, and PMID 39681070. A live search is available on PubMed.
The published TOL literature.
This section lists the published scientific literature on Targeted Osmotic Lysis for readers who want to review the primary sources directly. Targeted Osmotic Lysis is investigational and is not approved by the U.S. Food and Drug Administration, and its safety and effectiveness in humans are not established. Entries are ordered by evidence context, from a narrative review and a reference entry, to preclinical and animal studies, to individual human case reports. Each entry is labeled with its evidence type. This is educational information only and is not medical advice.
Targeted Osmotic Lysis: A Novel Approach to Targeted Cancer Therapies
Gould HJ III and colleagues. Biomedicines. 2022. Volume 10, Issue 4, Article 838. PMC9027517.
A narrative review in which the authors summarize the proposed TOL mechanism and prior findings on voltage-gated sodium channel activity in solid tumor cells. As the authors present it, this is a review of earlier work rather than a report of new original data.
Cancer as a Channelopathy. Appreciation of Complimentary Pathways Provides a Different Perspective for Developing Treatments
Gould HJ III and Paul D. Cancers. 2022. Volume 14, Issue 19, Article 4627. PMID 36230549. PMC9562872.
A review in which the authors argue that cancer can be understood as a channelopathy, a disease of ion channel regulation, and discuss what that framing might mean for treatment development. As the authors present it, this is a conceptual review of existing work rather than a report of new original data.
Targeted Osmotic Lysis in Cancer Therapies
Gould HJ III and Paul D. Encyclopedia (MDPI). 2022. Entry 23698.
A tertiary encyclopedia entry authored by Gould and Paul that summarizes the TOL concept for a general reference audience. As the authors present it, this is a secondary summary and not primary research.
Selective Lysis of Breast Carcinomas by Simultaneous Stimulation of Sodium Channels and Blockade of Sodium Pumps
Gould HJ III, Norleans J, Ward TD, Reid C, Paul D. Oncotarget. 2018. Volume 9, Issue 21, Pages 15606 to 15615. PMID 29643996. PMC5884651.
The earliest peer-reviewed report of the TOL concept. The authors describe experiments in cultured breast carcinoma cell lines and in mouse xenografts, and report that lysis tracked with the degree of sodium channel expression. As the authors present it, this is laboratory and animal work. It does not involve human subjects and does not establish safety or effectiveness in people.
Targeted Osmotic Lysis of Highly Invasive Breast Carcinomas Using Pulsed Magnetic Field Stimulation of Voltage-Gated Sodium Channels and Pharmacological Blockade of Sodium Pumps
Paul D, Maggi P, Del Piero F, Scahill SD, Sherman KJ, Edenfield S, Gould HJ III. Cancers. 2020. Volume 12, Issue 6, Article 1420. PMID 32486340. PMC7352419.
A laboratory and mouse study testing pulsed magnetic fields rather than direct electrical current as the stimulation source. The authors report reduced tumor size in treated mouse grafts and longer survival in one model compared with control groups. As the authors present it, these are findings in cell culture and in mice. Results in animals do not establish safety or effectiveness in people.
Targeted Osmotic Lysis: Killing Carcinomas Without Affecting Non-Cancerous Tissues
Journal of Pharmacology and Experimental Therapeutics. 2025. Meeting abstract 191249.
A preclinical study in cultured cells, published as a meeting abstract. The study authors report laboratory observations in cell culture. As a meeting abstract, it reflects early laboratory work with limited peer review and does not involve animals or human subjects.
Safety Evaluation of Targeted Osmotic Lysis Therapy in Beagles
Hunter RP, Randazzo JM, Miller PR, Paul D, Gould HJ III, Mallozzi R. American Journal of Veterinary Research. 2024. Volume 86, Issue 2. PMID 39681070.
A safety study in 12 healthy Beagle dogs, which the authors state was conducted to address the U.S. Food and Drug Administration Center for Devices and Radiological Health. The animals received three treatment cycles at two field strengths and were then examined. The authors report no adverse events attributed to exposure and no gross or microscopic lesions. As the authors present it, this study used healthy animals without tumors, included no untreated control group, and measured safety rather than any effect on cancer. It does not involve human subjects and does not establish safety or effectiveness in people.
The Role of Targeted Osmotic Lysis in the Treatment of Advanced Carcinoma in Companion Animals: A Case Series
Gould HJ III and colleagues. Case Reports in Veterinary Medicine. 2022. Article 2747108. PMC9363929.
A companion-animal case series in which the authors describe two cats and two dogs with advanced carcinoma. As the authors report the outcomes, no tumor was eliminated in any of the four animals, two showed a reduction in tumor size, one continued to grow, and three of the four animals were euthanized during or after the reported period. As the authors present it, this is uncontrolled veterinary observational data in a small number of animals and does not involve human subjects.
Emergency Use of Targeted Osmotic Lysis for the Treatment of Squamous Cell Carcinoma of the Cervix
Gould HJ III and colleagues. Current Oncology. 2021. Volume 28, Issue 3, Pages 2115 to 2122.
A single human case report authored by Gould and colleagues describing one patient. As the authors present it, a single case report describes one individual and cannot establish safety or effectiveness.
Use of Targeted Osmotic Lysis for the Treatment of Malignant Melanoma: Case Report
Gould HJ III and colleagues. Annals of Oncology Case Reports. 2025. Volume 5, Issue 1, Article 1027.
A single human case report authored by Gould and colleagues describing one patient. As the authors present it, a single case report describes one individual and cannot establish safety or effectiveness.
Every finding above is attributed to the authors of the cited work. A review article and an encyclopedia entry summarize prior work rather than report new results. Preclinical and animal studies do not establish safety or effectiveness in people. Individual human case reports describe single subjects and cannot establish effectiveness. Targeted Osmotic Lysis is investigational, is not approved by the U.S. Food and Drug Administration, and is not offered, arranged, or referred through this site. No claim of benefit, cure, superiority, or availability is made. This is educational information only and is not medical advice.
Common questions.
General questions about cancer and this resource.
General questions about cancer and about this resource. None of the answers below are medical advice.
Does this site offer or arrange cancer treatment?
No. FixCancer.org is educational. It does not offer, arrange, or refer anyone for treatment, it does not assess eligibility for anything, and it does not provide medical advice. People with questions about their own care should consult a licensed physician.
What is the difference between approved and investigational treatment?
An approved treatment has been reviewed by the U.S. Food and Drug Administration and found to be safe and effective for a specific use. An investigational treatment is still being studied and has not received that approval. Investigational findings, especially from laboratory or animal studies, do not establish safety or benefit in people.
What does it mean when cancer is “advanced” or “metastatic”?
Advanced cancer is a general term for cancer that is unlikely to be cured, often because it has spread. Metastatic cancer is cancer that has spread from where it started to other parts of the body. Metastatic cancer keeps the name of the original cancer. The right approach is individual and is decided with a licensed oncology team.
How do I find clinical trials?
Many U.S. trials are listed on ClinicalTrials.gov, a public registry maintained by the National Institutes of Health. You and your physician can search it by cancer type and location. Joining a trial is a medical decision made with your care team.
Where should I look for trustworthy cancer information?
Start with the National Cancer Institute (cancer.gov), the National Institutes of Health (nih.gov), ClinicalTrials.gov, the American Cancer Society (cancer.org), and PubMed. These are listed with links in the references section above.
How can I send a general educational question?
General, non-clinical questions about the published science are welcome by email through the contact link in the footer. This is not a clinical intake and no eligibility is assessed. No medical advice is provided, and no protected health information should be sent. For medical decisions, consult a licensed physician.
Questions about Targeted Osmotic Lysis.
Targeted Osmotic Lysis is an investigational, research-stage mechanism described in the published literature. It is not approved by the U.S. Food and Drug Administration, its safety and effectiveness in humans are not established, and it is not available as a treatment. The answers below are educational information only and are not medical advice.
What is Targeted Osmotic Lysis (TOL)?
Targeted Osmotic Lysis is an investigational, research-stage mechanism studied in laboratory and veterinary models. The published hypothesis is that it disrupts cancer cell water balance without using chemotherapy, radiation, or surgery. It is not FDA approved, and its safety and effectiveness in humans are not established. The published citations are listed in the literature section of this site and can be verified independently.
Does TOL use chemotherapy or radiation?
In the published preclinical and veterinary research, the TOL mechanism is described as not introducing cytotoxic chemotherapy agents, not using ionizing radiation, and not requiring surgical resection. This describes the studied mechanism only. TOL is investigational and not FDA approved, and its safety and effectiveness in humans are not established. This is educational information, not medical advice.
What human data exist?
The human evidence is limited to individual case reports. One is indexed in PubMed. Two others appear in a journal that is not indexed in PubMed or MEDLINE. Case reports cannot establish effectiveness. There are no published randomized trials and no human trials registered on ClinicalTrials.gov. This site does not report patient counts or outcomes, and it is educational, not a clinical record.
What cancers has TOL been studied in?
The published research describes laboratory and veterinary study of stage 3 and stage 4 solid tumor carcinomas across several tissue types. This is research context only. It is not a statement that TOL treats any cancer in humans, and it is not an eligibility criterion.
What about bone cancers and blood cancers?
The published rationale focuses on solid tumor cells. Bone-based and blood-based cancers are described in the literature as outside that rationale. Any further research would be early-stage. This is educational information only.
Does this site arrange treatment or referrals?
No. This site is educational and does not offer, arrange, or refer anyone for treatment, and it does not screen for eligibility. People with questions about their own care should consult a licensed oncologist and review the published primary-source literature cited on this site.
Where to find reliable information.
Cancer information online varies widely in quality. For trustworthy, plain-language material, start with established government and nonprofit sources. These organizations review their content with medical experts and update it regularly.
- National Cancer Institute (cancer.gov), the U.S. government’s principal cancer information service.
- National Institutes of Health (nih.gov), the parent biomedical research agency.
- ClinicalTrials.gov, the public registry of clinical studies.
- American Cancer Society (cancer.org), patient-focused guides and support.
- PubMed (pubmed.ncbi.nlm.nih.gov), the index of peer-reviewed biomedical literature.
When you read about a treatment, ask whether it is approved or investigational, what kind of evidence supports it, and whether the source is trying to sell something. Bring anything you find to your own care team before acting on it.
References for this page.
The general cancer education on this page is drawn from the following public sources. Links are provided so readers can verify each one.
- National Cancer Institute. “What Is Cancer?” cancer.gov/about-cancer/understanding/what-is-cancer
- National Cancer Institute. “Cancer Staging.” cancer.gov/about-cancer/diagnosis-staging/staging
- National Cancer Institute. “Metastatic Cancer.” cancer.gov/types/metastatic-cancer
- National Cancer Institute. “Types of Cancer Treatment.” cancer.gov/about-cancer/treatment/types
- National Cancer Institute. “Clinical Trials Information.” cancer.gov/about-cancer/treatment/clinical-trials
- U.S. National Institutes of Health. ClinicalTrials.gov. clinicaltrials.gov
- American Cancer Society. cancer.org
- U.S. National Library of Medicine. PubMed. pubmed.ncbi.nlm.nih.gov
Educational Inquiry
For clinicians and researchers.
This site is educational and does not accept patient referrals or arrange treatment. Clinicians and researchers with general questions about the published science are welcome to write. No medical advice is provided and no protected health information should be sent.
The statements on this site, and any products or therapies referenced, have not been evaluated or approved by the U.S. Food and Drug Administration. This content is for general educational and informational purposes only. It is not medical advice and is not a substitute for professional diagnosis or treatment. Nothing here is intended to diagnose, treat, cure, or prevent any disease. No product or therapy is offered, sold, or promoted through this site, and individual results are not implied or guaranteed. Always consult a licensed healthcare provider before making decisions about cancer care.